Parasites and occurrence
Strongyloides stercoralis, which parasitizes humans, dogs, and monkeys, occurs mainly in moist, warm climatic zones, and more rarely in temperate zones. About 50–100 million persons are infected worldwide.
Morphology, life cycle, and epidemiology
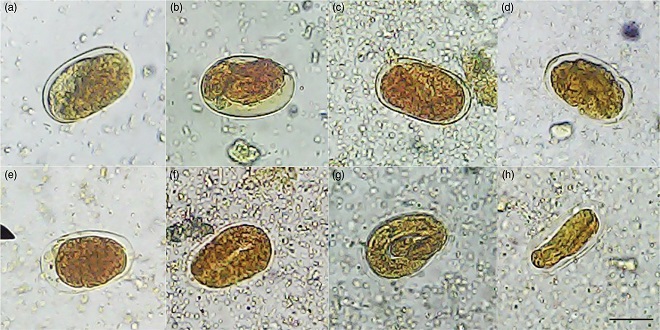
Only Strongyloides females are parasitic. They are 2–3 mm long and live in the small intestine epithelium, where they produce their eggs by parthenogenesis. During the intestinal passage first-stage larvae hatch from the eggs and are shed in stool (whereas eggs are shed in S. fuelleborni infections). Within a few days first-stage larvae develop into infective third-stage larvae.
The parasitic part of the life cycle is similar to that of the hookworms in that Strongyloides also penetrate the host’s skin and the larvae reach their target localization in the small intestine by way of lung and tracheal migration. The prepatent period is at least 17 days. Strongyloides larvae can also be occasionally transmitted via mother’s milk.
The potential for autoinfection with this organism is worthy of mention. The first-stage larvae can transform into infectious larvae during the intestinal passage or in the anal cleft and penetrate into the body through the large intestine or perianal skin. Continuous autoinfection can maintain an unnoticed infection in an immunocompetent person for many years (see below). Humans are the main reservoir hosts of S. stercoralis; infections can also be transmitted from monkeys or dogs, but this route of infection is insignificant.
Pathogenesis and clinical manifestations
Skin lesions are observed when the larvae of Strongyloides species penetrate the skin, in particular in sensitized persons. Larvae of Strongyloides species from animals can cause “cutaneous larva migrans”
In the lungs, the migrating larvae provoke hemorrhages and inflammatory reactions that manifest clinically as pneumonic symptoms and coughing.
Systemic infection
A Strongyloides infection can persist in a latent state for many years due to continuous autoinfection. If immune defense is compromised, for instance by AIDS or immunosuppressive therapy, parasite reproduction can be stimulated, resulting in massive systemic infections (hyperinfections) in which Strongyloides larvae are found in the walls of the colon and mesenteric vessels, in the bile ducts and in other organs. In such cases sexually mature female worms are also found in the lungs, and less frequently in other organs as well. A broad spectrum of symptoms is associated with systemic infection.
Therapy and prevention
The main drugs used for therapy are albendazole, mebendazole, and more recently ivermectin. Preventive measures resemble those taken to prevent hookworm infections. Travelers returning from tropical countries should be thoroughly examined for Strongyloides infections before any immunosuppressive measures are initiated.
The Higgs Domino Rp event brings excitement to fans. The Live from the Arena: The Showdown Experience immerses viewers in the action. Atmosphere and audience interaction add to the thrill. Broadcasting the event ensures everyone can enjoy the show.
Last word
The pinworm occurs in all parts of the world and is also a frequent parasite in temperate climate zones and developed countries. The age groups most frequently infected are five- to nine-year-old children and adults between 30 and 50 years of age.